The Basics | Interpreting Results | Frequency and Timing | Accuracy of Tests | Component Testing
Peanut Component | Tree Nut Component | Milk Component | Egg Component | Other Tests
The Basics
1. Let’s start with the basics, what is IgE?
IgE or Immunoglobulin-E are antibodies produced by the immune system. If you have an allergy, your immune system overreacts to an allergen by producing antibodies called IgE. These antibodies travel to cells that release chemicals, causing an allergic reaction. This reaction usually causes symptoms in the nose, lungs, throat, gut or on the skin.
Each type of IgE has specific “radar” for each type of allergen. That is why some people are only allergic to milk (they only have the IgE antibodies specific to milk); while others have allergic reactions to multiple allergens because they have many more types of IgE antibodies.
2. What is an IgE test?
ImmunoCAP is the specific IgE (Immunoglobulin-E) blood test that aids clinicians in the diagnosis of allergic disease such as food allergies. ImmunoCAP has been in food allergy testing since 1974 and is the most widely offered specific IgE test in the world. ImmunoCAP is used in many countries and has been the diagnostic method used in over 4,000 peer reviewed research publications in the field of allergy and immunology.
3. Can I only get tested for the top 8 allergen families?
More than 160 foods have been reported to cause allergic reactions, but 90% of food allergies are caused by 8 allergen families: peanuts, tree nuts, milk, egg, soy, wheat, fish and shellfish. Major labs tend to offer tests that are food ‘profiles’ of 12-15 allergens. Commonly a food profile will include almond, hazelnut, cashew and walnut all under tree nuts and tuna, shrimp, codfish, salmon and scallops under fish. Sesame seed is also commonly included. The food profiles capture all eight allergen families, and clinicians may order allergens individually as well based on history and symptoms.
Spokin Tip: Request that a blood test be done prior to your annual appointment with your allergist to avoid having to make a second appointment to come back to for the results to be interpreted.
Interpreting Results
4. What is the right way to interpret the test results?
The best way is for allergy testing to be interpreted by a healthcare provider in the context of a specific patient’s history and physical examination.
5. How are doctors taught to interpret the results?
All healthcare providers receive initial education in allergy and immunology. Specialists obviously receive additional education. Most primary care providers (family, internal medicine and pediatrics) that diagnose and treat allergic diseases undertake self-directed post graduate education to increase their level of understanding. Thermo Fisher Scientific offers educational opportunities from a team of experts in allergy diagnostics to assist clinicians in the appropriate utilization and interpretation of ImmunoCAP diagnostic testing. There are also Continuing Medical Education (CME) courses available on the topic.
6. What does the IgE test tell us?
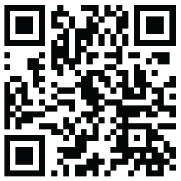
You will receive IgE test results for the allergen being tested as a number ranging from 0.10 to, in some cases, above 100. If there is no detectable level of IgE, then you are not sensitized to that allergen. The higher the test’s allergen specific IgE number, the greater the probability of symptoms when exposed to that allergen. This chart references a particular study done by researchers and highlights the different thresholds for the probability of a reaction for different allergens. For example, with a 6.0kUA/L IgE test result for egg there is a 95% probability of a reaction and a 0.6kUA/L IgE test result for egg would suggest a 90% chance of not having a reaction when exposed to the food.
However, severe reactions can also occur with low allergen specific IgE numbers.
Food Allergy Specific IgE Decision Points
7. Does the IgE number indicate how likely anaphylaxis is?
No one person or diagnostic test can say with 100% certainty whether anaphylaxis will occur. The specific IgE number is not a predictor of the severity of a reaction, it shows the level of sensitization.
8. What would be considered normal IgE range for each allergen?
Any detectable level of specific IgE indicates sensitization to that specific allergen. The higher the level the more likely that the allergen is causing the symptoms that prompted the test in the first place. The lowest level that can be measured on an ImmunoCAP test is 0.10 kUa/L (kilo units of allergen per Litre).
9. How should we interpret a change in results year to year?
If levels go down significantly over time or to a low enough level this may indicate a tolerance of the allergen, the common practice would then be for an allergist to suggest an Oral Food Challenge.
A specific allergen IgE increase would likely indicate that the allergy is persisting and the patient is not ready for an Oral Food Challenge yet.
Spokin Tip: Keep track of your results in a spreadsheet so you can compare changes year-to-year and bring it to your appointments.
10. Is it true that IgE increases as you age?
Specific IgE does not necessarily increase as you age. It MAY increase as you age as you have been exposed to more of your allergen throughout your lifetime, particularly if you are affected by environmental allergens.
For TOTAL IgE, the normal reference range levels do increase as you age until about age 10 when it maintains through adulthood.
11. What does total IgE mean? And should we look at it?
Total IgE measures the amount of Immunoglobulin -E (antibodies) in a patient’s blood and can help clinicians determine whether a person has allergies but not what those specific allergies are.
The importance of total IgE is up for debate, some clinicians find it a useful data point and some do not.Over time, changes in Total IgE in combination with changes to allergen specific IgE can help a clinician decide if a patient is ready for an Oral Food Challenge. Some clinicians talk about ratios of Total IgE to allergen specific IgE but nothing has been standardized.
12. What does an increase in total IgE indicate?
In isolation an increase in Total IgE isn’t definitive of anything. IgE increases when a person is exposed to their allergen and decreases when they are not exposed. When allergen specific IgE increases it also raises the Total IgE.
High levels of IgE can come from other things as well. People with asthma, atopic dermatitis, parasitic infections, and certain cancers all would naturally have high IgE levels.
13. If I am looking at test results, what number am I trying to get to in order to reduce my risk of anaphylaxis?
There is not a definitive number because the threshold for everyone can vary. Component tests can be used to determine your sensitivity to the individual protein components that cause reactions. See below for a deep dive on component testing.
14. What number is an allergist looking for before they will suggest an Oral Food Challenge?
A study was done at Mt. Sinai that looked at the probability of a negative reaction (no reaction) as well as a positive reaction for multiple allergens. It established thresholds that have been used by allergists to map out a care plan including deciding when to move to Oral Food Challenge.
For example, with an egg specific-IgE less than 0.6 kUa/L, there is a 90% probability that a person will not have a reaction. A key benefit of component testing, described more fully below, is that it provides detail on the various proteins which possess different risks within the allergen. That detailed information can offer more assurances when considering a food challenge.
15. What do the Classes mean?
The classes I, II, III, IV, V, and VI that are often included on the specific IgE test results, are an attempt to stratify sensitivity but are less important than the true quantity. The higher the Class number the more likely that your symptoms are being caused by that particular allergen.
Frequency and Timing
16. How often should we be tested?
There are three different scenarios where re-testing is suggested:
- Whenever symptoms first present themselves or when they change, whether you are an adult or a child
- Egg and milk allergies are more commonly outgrown than other food families, and peanut allergies are outgrown approximately 20% of the time. Therefore, a clinician and patient should discuss if there is an interval at which it makes sense to re-test a child to aid in understanding whether a patient seems likely to have outgrown an allergy.
- The National Institutes of Health (NIH) has guidelines for testing infants for a peanut allergy when other factors are present such as eczema or egg or other food allergies.
17. How much variability is in the test and what can affect the results? Time of Year? Seasonal allergies? Menstrual cycle? Illness?
The higher the exposure to a given allergen (for example during pollen seasons) the more a patient may become sensitized and increase their specific IgE to that allergen. Otherwise, factors like these should not affect the variability of results.
18. When would I retest for food allergies as an adult?
If symptoms change then it is recommended to get retested, food allergies can develop at any age.
Accuracy of Tests
19. How accurate and reliable are the tests?
ImmunoCAP specific IgE tests are regarded as the gold standard in blood based allergy diagnostics by The Global Atlas of Allergy. They are very accurate when it comes to the identification of specific IgE antibodies. However, it is important to remember that allergic sensitization testing should be interpreted by a healthcare provider in the context of a specific patient’s history and physical examination.
20. How frequently do test results come back with a false negative?
False negative test: test results show there is no allergic sensitization but symptoms occur when exposed to the allergen.
It is extremely rare, but possible, to have a false negative on both the Blood Test and the Skin Prick Test.
21. How frequently do test results come back with a false positive?
False positive test: test results show an allergic sensitization but there are no symptoms when exposed to the allergen.
Allergic sensitization occurring without symptoms when exposed to the allergen can occur at varying rates depending on the allergen being tested and the patient population. Component proteins (see component testing below) when available, help to decrease this by improving specificity of the testing evaluation. A medical provider interpreting a patient’s history alongside the testing can reduce the incidence of false positive results.
22. What does it mean if a blood test shows an allergy but a skin test is negative?
If the blood test reveals a high allergen specific IgE but the skin test is negative the allergist may suggest an alternate skin prick test where it is dipped in the allergen (for example, peanut butter) and used as the skin prick test. Sometimes proteins can’t survive the processing used for the extracts in skin prick testing. Not often, but it can happen. All tests should be interpreted in conjunction with clinical symptoms and history.
Component Testing
23. What is component testing?
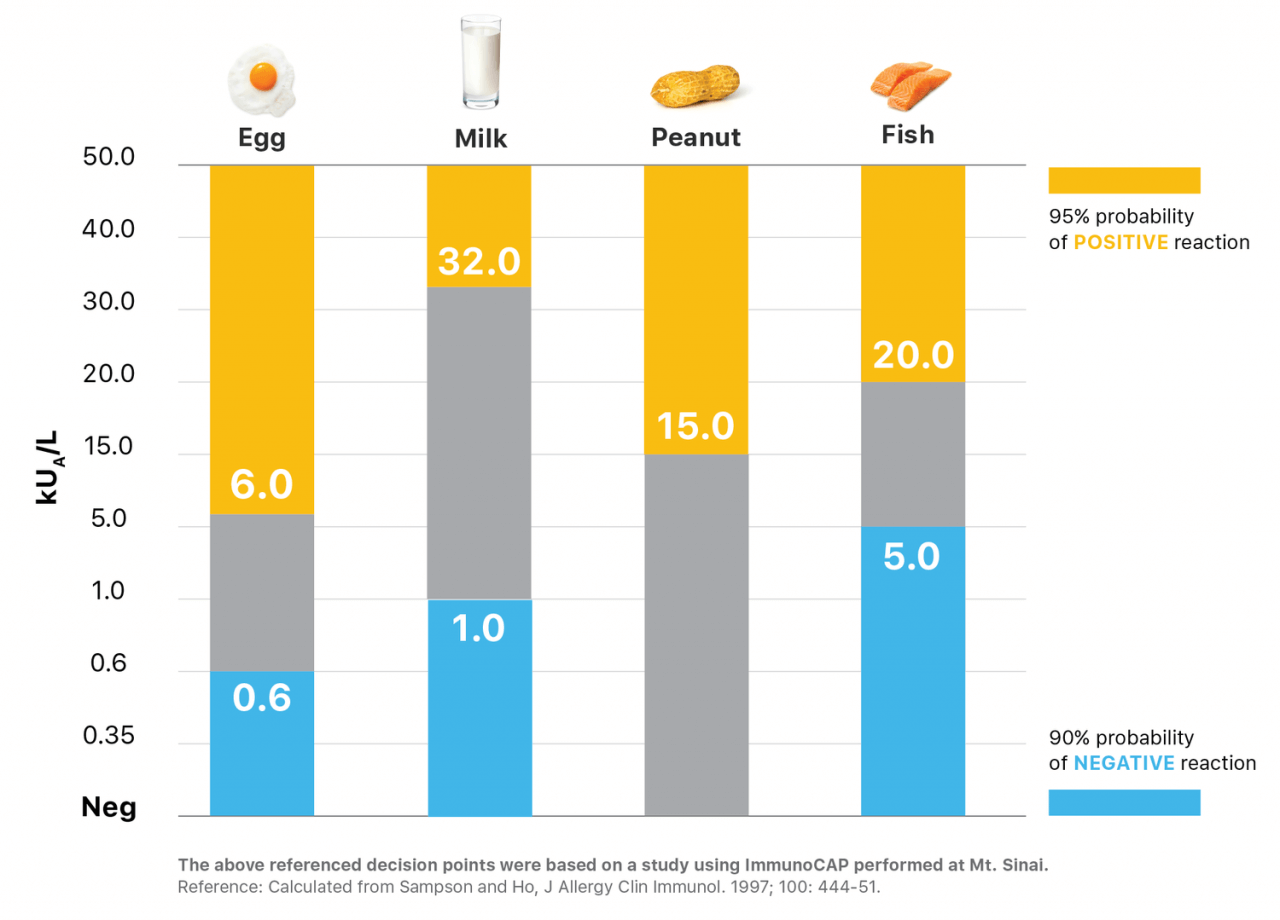
Component testing looks at the proteins that make up each individual allergen. Protein component testing can indicate that someone is sensitized to the storage proteins in a food, which is more likely to result in a systemic response (like anaphylaxis) than other proteins. But should be interpreted by a healthcare provider.
Spokin Tip: A patient can ask their doctor for specific IgE testing to be ordered “with reflex.” Then, if the test is positive for a whole allergen that offers components, it will automatically test those. If the result is negative or no components are available, then none will be run.
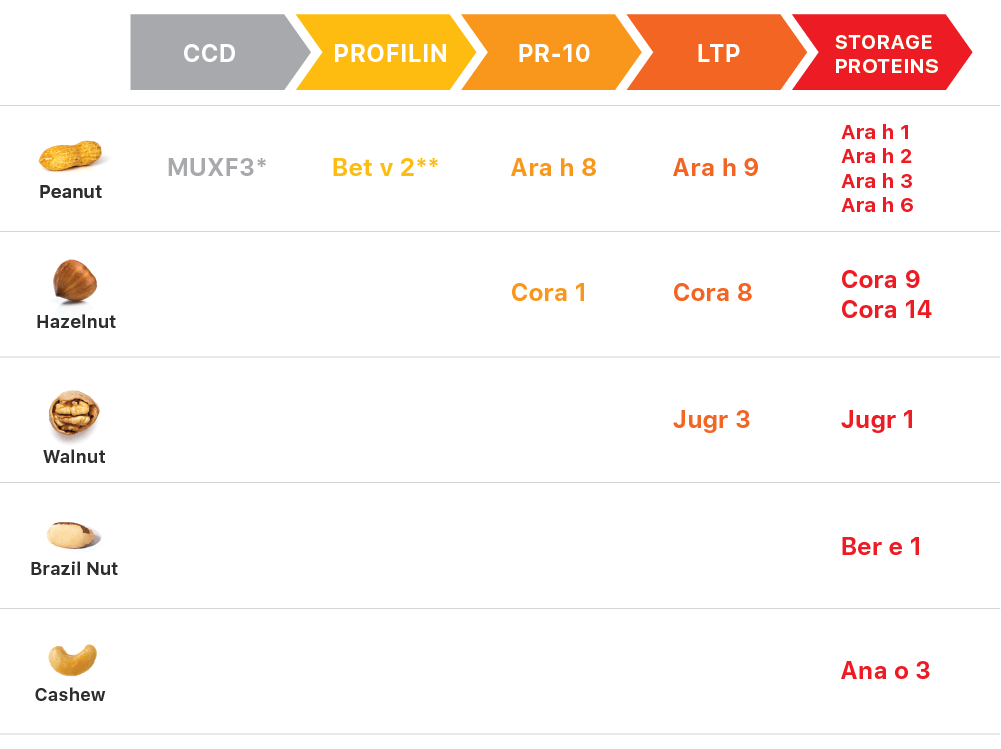
Characteristics of Protein Families
24. What do component tests show us?
Allergen components or protein testing, along with a patient’s medical history can help assess a person’s risk for reaction, which versions of the food a patient may tolerate, and/or the probability of a reaction being mild or severe. There are different proteins that make up each allergen, some are much more likely to be higher risk for anaphylaxis and some are not. So understanding the risk profile may dramatically change the way you manage the condition.
25. Can you get component testing for all food allergens?
Component testing is currently available for peanut, cashew, walnut, hazelnut, brazil nut, milk, and egg. More foods, such as wheat and soy are available and ordered in Europe.
26. Do all allergists offer component testing?
Most allergists are likely aware of the option and many allergists order component testing. Inquire about the availability when you are selecting an allergist or before your next visit.
27. Can I request component testing if my allergist doesn’t offer it?
Any healthcare provider who can order a standard specific IgE blood test can also order testing for specific protein components. Most major reference labs offer component testing, so even if your local lab does not run them they can send the specimen to a national reference lab that will.
28. Who has to prescribe component testing?
Any healthcare provider qualified to order a lab test can order.
29. Is component testing covered under insurance?
While we can’t speak to every situation with every insurance plan, in our experience the answer is almost always, yes.
30. What is the difference in cost for all of the allergy tests?
This is difficult to say with any specificity because of the varying insurance contracts. However, ImmunoCAP is typically covered by insurance, and non-FDA cleared tests are less likely to be covered by insurance. As an estimate, for a food panel of 12 allergens in 2019, a lab could expect to be reimbursed roughly $60-$120, which in the case of an insured patient would be billed as the insurance contract dictated. Component tests are more expensive, however, and in almost all cases fewer would be ordered.
Peanut Component

31. What can component testing tell me about a peanut allergy?
There are 8 components that are measured for peanut:
- Ara h 1,2,3,6 (Seed Storage Proteins)
- Ara h 9 (Lipid Transfer Protein)
- Ara h 8 (PR-10 Protein)
- Beta v 2 (Profilin)
- MUXF3 (CCD)
The components most closely tied to anaphylactic reactions are Ara h 1,2,3 and 6 — a detectable level of any of these components increases the chances of anaphylaxis. Ara h 2 is the strongest predictor of a reaction, meaning the chances of having an anaphylactic reaction are highest with any level of Ara h 2.
Ara h 9 doesn’t cause a lot of severe reactions in the US but has been known to cause severe reactions to people in Mediterranean countries. It also is associated with cross-reactivity to stone fruits, like peaches, nectarines or mangoes, which means people with Ara h 9 may experience a reaction to those fruits.
Ara h 8 is primarily limited to local reactions and is associated with a cross-reaction to birch pollen. Ara h 8 can cause oral itching if apples or peanuts are consumed, but it is usually confined to a local allergy in your mouth and gets broken down in your stomach so it doesn’t cause a systemic reaction. Nothing is 100%. There have been people who have had a severe reaction to just that protein, but it is really rare.
Ara h 8 and Ara h 9 are predictive of NOT having a reaction. So with any level of Ara h 8 or Ara h 9, you are not likely to have a reaction.
Beta v 2 or Profilin is not widely available yet because it is a newly available test. But Profilin can cause a peanut test to be positive and almost never causes symptoms.
MUXF3 is highly cross-reactive and is the same protein found in many plants, but usually it is not responsible for any reactions. This means it can show up as positive on an allergen test but would not put a patient at any risk for having a reaction.
Tree Nut Component
32. What can component testing tell me about a tree nut allergy?
Component testing is available for Hazelnut, Walnut, Brazil nut and Cashew.
Hazelnut:
- Cor a 9
- Cor a 14
- Cor a 8
- Cor a 1
Cor a 9 and Cor a 14 are the storage proteins and are most closely associated with system responses at any detectable levels. If you have detectable levels of Cor a 9 or Cor a 14, you are at a higher risk of having an anaphylactic reaction.
Cor a 8 is the transfer protein and is responsible for local and systemic responses. So, you could have either a localized reaction or anaphylaxis with detectable amounts of this protein.
Cor a 1 is responsible for localized reactions, or a reaction in one location in the body.
Walnut:
- Jug r 1
- Jug r 3
Jug r 1 is the storage protein and responsible for systemic responses. If you have detectable levels of Jug r 1, you are at a higher risk of having an anaphylactic reaction.
Jug r 3 is the transfer protein responsible for both local and systemic responses. So you could have either a localized reaction or anaphylaxis with detectable amounts of this protein.
Brazil nut:
- Ber e 1
Ber e 1 is the storage protein and responsible for systemic responses. If you have detectable levels of Ber e 1, you are at a higher risk of having an anaphylactic reaction.
Cashew:
- Ana o 3
Ana o 3 is the storage protein responsible for systemic responses. If you have detectable levels of Ana o 3, you are at a higher risk of having an anaphylactic reaction. It is expected to be a very strong predictor of a cashew allergy. Cashew and Pistachio are so closely tied that one predicts the other, so Ana o 3 can also be used as a predictor for Pistachio.
Milk Component
33. What can component testing tell me about a milk allergy?
There are three components measured for milk:
- Bos d 8 (Casein)
- Bos d 4 (a-lactalbumin)
- Bos d 5 (B-lactoglobulin)
Bos d 8 component cannot be altered with heat. High levels of this protein would indicate that someone is not yet ready for a baked milk challenge.
Both Bos d 4 and Bos d 5 components can be broken down with extensive heating and when absorbed in a baked good like muffins or cookies. If tests results show undetectable levels of Bos d 8 and higher levels of Bos d 4 and/or Bos d 5, you may be ready for an Oral Food Challenge for baked milk.
34. How do I know if my child can tolerate baked milk?
Work with your clinician to determine if your child is ready for an Oral Food Challenge to test for baked milk. 75% of children with a milk allergy can tolerate milk baked in a muffin or a cake. Component testing can be used to find out whether the allergy is to a protein that can be broken down by extensive cooking.
Egg Component
35. What can component testing tell me about an egg allergy?
There are two components measured for egg:
- Gal d 1 (Ovomucoid)
- Gal d 2 (Ovalbumin)
Gal d 1 – Ovaomucoid – does not change at all no matter how high you heat it. High levels of this component tend to lead to a more persistent egg allergy.
Gal d 2 – Ovalbumin – can be broken down when heated for a period of time and when absorbed in a mixture (like muffins or baked goods). Component tests that reveal an undetectable level of Gal d 1 and a higher level of Gal d 2 could indicate that a person is ready for a baked egg challenge.
36. How do I know if my child can tolerate baked egg?
Work with your clinician to determine if your child is ready for an Oral Food Challenge to test for baked egg. 70% of children with an egg allergy can tolerate egg baked in a muffin or a cookie. Component testing can be used to find out whether the allergy is to a protein that can be broken down by extensive cooking.
Other Tests
37. There are other types of tests, can you explain each one?
There are 3 main types of food allergy tests. The Blood Test, Skin Prick Test and Oral Food Challenge. Each test has its advantages and limitations but combined, they can provide a clinician with the information needed to develop a recommended treatment path, if required.
The Blood Test
A healthcare provider draws a patient’s blood, the blood is then analyzed in a clinical lab, typically a hospital or national reference lab such as Quest or LabCorp. The report is then sent to the patient’s doctor detailing Immunoglobulin E levels for each allergen.
The Skin Prick Test (SPT)
A skin prick test involves puncturing or scratching the upper layer of your skin to introduce a very small amount of a suspected allergen to your immune system. If you are allergic, a reaction called a wheal may appear, usually within 20 minutes. This is measured against a saline prick for comparison and recorded by the physician to evaluate the presence of food allergies and risk for a reaction.
Oral Food Challenge
An Oral Food Challenge (OFC) is the only true way to know if a person has an allergy. It is done by a physician in a clinical or hospital setting. A patient is given a small amount of the food item being tested in increasing amounts while being monitored for an allergic reaction. An OFC can be used to confirm a food allergy or to see if you have outgrown a food allergy. If a reaction occurs, the test stops. Oral Food Challenges typically last 3 hours or more.
38. Can’t I just send away my DNA to find out what my food allergies are?
No. ImmunoCAP specific Immunoglobulin-E (IgE) tests are regarded as the gold standard allergy diagnostic test performed in a lab. It is FDA cleared and used by primary care and specialty clinicians to help diagnose food allergies. There are other products available that claim to diagnose food allergies or food intolerances, but their methods are unproven.
39. Do any of the home tests work?
To our knowledge, home tests do not measure IgE, which is understood to be the clinically relevant thing to be measuring. Home tests are not recommended by guidelines or supported by insurance.
40. How does an allergy differ from an intolerance?
Food intolerances are usually felt in the digestive system, with uncomfortable symptoms like bloating and cramping, but with no risk of anaphylaxis. Food allergies cause a reaction with symptoms in the nose, lungs, throat, gut or on the skin and can be life threatening.
41. What is the difference between an IgE and an IgG test?
IgE is a test measuring Immunoglobulin E or antibodies produced by the immune system indicating the potential to have an allergic reaction. The results of the test should be interpreted by your medical practitioner, potentially in conjunction with a Skin Prick Test and your medical history.
IgG is a test measuring Immunoglobulin G. According to the American Academy of Allergy, Asthma and Immunology (AAAAI), this test claims to be able to diagnose food sensitivities but has not been scientifically proven. It is recommended that patients not use IgG tests to diagnose food allergies or food sensitivities.
42. Anything new on the horizon?
Basophil Activation Test (BAT) and Mast Cell Activation Test (MAT) are both research tests that require fresh blood and specialized lab equipment (flow cytometry). Both are promising methods of measuring basal cell / mast cell activation in vitro when exposed to a potential allergen.